The Free Lunch
ã
Neal Henderson [nealhe@home.com]
Train while sleeping!
Have you seen the advertisements for Hypoxic Tents and Hypoxic Rooms? Colorado Altitude Training http://www.altitudetraining.com/ and Hypoxico http://www.hypoxictent.com/ are two that come to mind.
Each of these sites has articles about altitude training and athletic performance.
The list of athlete’s on the Hypoxic Tent webpage is impressive: Michellie Jones, Simon Lessing, Heather Fuhr, Paula Newby-Fraser, Peter Reid, Jan Rehula, Rob Barel, Siri Lindley, Greg Welch, Mieke Suys, and that is just part of the listed athletes.
Get a 3% to 6% speed improvement while you sleep. Wow! Is it legal? Yep, so far anyway. Does it work?
Two questions:
One - Does putting your body in a reduced oxygen atmosphere trigger a physical adaptation to increase the oxygen carrying capacity of the body? Yes, two of the common measurements of blood oxygen carrying capacity are hematocrit and hemoglobin, and each measure (from the common CBC – Complete Blood Count test) can be increased by living in a reduced oxygen environment. The kidneys and the liver sense lower oxygen pressure, and then secrete a hormone (85% kidney produced), EPO, erythropoietin, which in turn activates bone marrow to produce more red blood cells. This effect is well documented in medical literature.
Recombinant EPO is a synthetic version of this hormone sold under various names such as epogen, procrit, and eprex used for treating anemia and other disorders.
Two – Does increased hematocrit (ratio of red blood cells to total plasma in body) improve athletic performance at sea level? The answer is a provisional Yes. The few articles and studies that have been done report a link between increased hematocrit/hemoglobin and increased performance (running speed) of 3 to 6%. Judging from the number of athletes getting disqualified for excess hematocrit, it is a reasonable supposition that improved oxygen carrying capacity in the blood is believed to improve performance.
Velo News stated that a blood specialist called as a witness on behalf of disqualified Italian cyclist Marco Pantani conceded Friday that the former Tour de France champion had given a reading of 60.1 percent red blood count in medical tests but denied the rider had taken banned substance EPO. He quickly added, however, that the fact Pantani had been training at altitude in Colombia, the intensity of the race, the trauma to his body of the crash and the way in which the sample was taken could all help explain the anomaly. Training at 2500m in the Andes, Tura maintained, "would have provoked a raising of four percent, which would have brought it to 49". Tura said that he believed that would have been the rider's level at the start of the race.
The max limit for hematocrit by the ICU - the Union Cycliste Internationale http://www.uci.ch/ - is 50%. The max limit for hemoglobin by the FIS - Federation Internationale de Ski http://www.fis-ski.com/splash/default.sps - is concentrations of 16.5 g/dl women and 18.5 g/dl men. USA Triathlon http://www.usatriathlon.org/ uses the provisions of the United States Olympic Committee's National Anti- Doping Program ("NADP"), which state that you cannot inject EPO or blood pack (transfuse blood) but have no max limits on hematocrit or hemoglobin Steve Locke, Executive Director USA Triathlon, Steve@USATriathlon.org said that currently there are no restrictions on using hypoxic tents or rooms or actually going to altitude to increase blood oxygen carrying capacity.
I was curious about the first question – could I increase my blood oxygen carrying capacity? Would altitude training work for me?
Keep in mind this is an anecdotal experience, done by an amateur, with no medical credentials. No double blind tests, no controls, just my data.
In August 2000 I went to the mountains to test how altitude training would work for me, a 67 year old guy. Before trying a hypoxic tent I wanted to measure the effects of altitude with Mother Nature. Besides, my wife said she isn’t sleeping in some weird plastic tent or oxygen deprived room.
Before leaving I arranged with my doctor to have a blood test and periodic follow up blood tests, using the common test called a CBC or Completed Blood Count. (About $60 a pop at Palomar Hospital Lab in Escondido, CA.)
I spent 9 nights at 8,300 to 12,500 ft and some of the days, with my trusty Polar heart monitor and hiked, biked, and ran at different altitudes from 4,000 ft to 14,246 ft (White Mountain, CA).
My previous experience at altitude was usually in controlled environments (except for treks like Mt. Rainier) in an airplane when I was working as an airline pilot. I also spent time in a military low pressure chamber where we experienced how goofy we would get with a lack of oxygen and experimented with grunt breathing at 37,000 ft. to stay conscious. When I was flying single engine military aircraft I used to watch flies caught in the cockpit roll on their backs when I depressurized the cockpit at 35,000 ft, only to come back to life again after landing when the pressure increased. Flies are tough.
I kept a simple journal of my experiences at altitude:
1 Aug – Drove to Lone Pine & Whitney Portal 8,300 ft. Sleep 12 hrs (hours) - Put my food in the bear locker. No altitude sickness – felt good. A bear tore a window out of the car by me and ripped out some of the upholstery looking for food. Local newspaper reported that rangers killed the bear 2 days later.
2 Aug - Drove to Univ Calif Barcroft Lab - 22 miles 4WD dirt road. (Prior permission required, locked gate) – 12,500 ft. Sleep 11 hrs - Slight headache and nausea from altitude. Big lightning storm with bolts hitting right next to car. Didn’t want to be found next day as a French fry in the car so got invited to sleep in the student dormitory in the big metal Quonset hut of the lab (with lightning rods). Sleeping pulse 70 (usually 42 at sea level) Heart beat noticeable. Sitting pulse 67 Oxygen saturation 91%.
3 Aug – Barcroft Lab – 12,500 ft Sleep 11 hours Waking pulse 57. Bit of diarrhea Hike summit White Mountain 12,426 ft at HR (heart rate) 124-133. Big thunderstorm with marble sized hail – lightning too close – ran downhill some to hurry – HR 153 - lower areas covered with hail – beautiful views
4 Aug – Slept 11 hrs in campground 9,000 ft (closer to Bishop so I could bike at 4,000 ft – sleep high, train low) Wake pulse 60
5 Aug – campground 9,000ft Wake pulse 50, Slept 11 hours. slight amount of blood when blowing nose. Project director for Bristlecone Pine Tree Ring Lab (oldest trees in world) made presentation at campfire.
6 Aug – campground 9,000 ft Wake pulse 52, Slept 11 hrs, Bike 1.8 hrs, hot 105F, some hills, HR 124-144, pulse slow to recover, 30 min to HR 74.
7 Aug Campground 9,000 waking pulse 54, slept 11 hours, Fast hike of Bristlecone Forest at 10,000 to 10,8000 ft - 2 hrs – 2 different loops – HR 100 – 130.
8 Aug Campground 9,000ft forgot pulse slept well 9 hrs, bike 2.75 hrs hills - temp 90F HR 125-140. Visited Caltech Radio Astronomy site.
9 Aug Barcroft Lab 12,500 ft slept 10.5 hrs could feel heart thump but no altitude sickness symptoms.
Hiked White Mountain summit again. HR 107 – 120. Felt very tired afterwards.
10 Aug Barcroft Lab 12,500 ft Slept 11.75. Slept very well. Seem to be acclimated now. Waking pulse 50. Drove home to Escondido for blood test.
A few comments about the experience. First – gradual acclimatization to altitude is important. I had a slight headache and very slight nausea the first night at 12,500 ft. The second night at 12,500ft I slept well but was conscious of my heart beating and a higher heart rate than normal. The rule of thumb is when above 9,000 to 10,000 ft sleep only 750 to 1,000 ft higher each night. By the end of 9 days I was quite comfortable sleeping at 12,500 ft. Also physical fitness doesn’t have much effect on how you will be affected by altitude sickness. At higher altitudes climbing too rapidly can result in death from HAPE (High Altitude Pulmonary Edema) and HACE (High Altitude Cerebral Edema). Further reading - Altitude Illness, Prevention and Treatment, Stephen Bezrechka, MD 1998 Published by The Mountaineers. (Available through www.amazon.com )
My usual waking pulse is 42 and at altitude it was a lot higher the first few days, gradually settling about 8 to 12 beats higher than sea level. My max pulse on a sea level EKG treadmill test was 176 and the highest pulse I saw (high intensity effort climbing) was 165 at altitude, similar to a high intensity effort pulse at sea level.
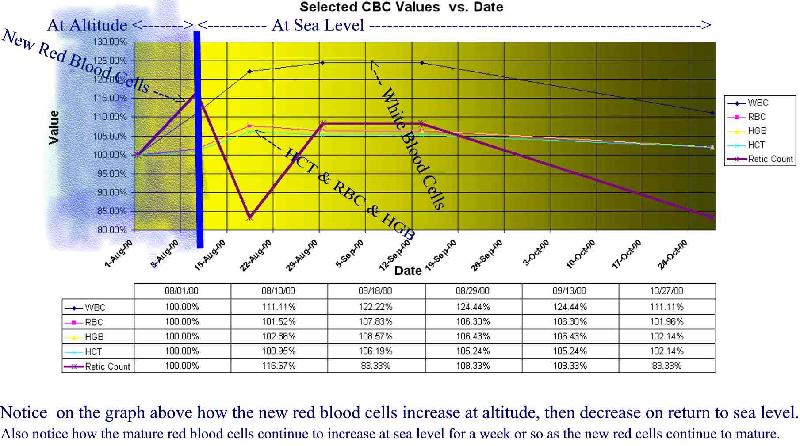
In 9 days at altitude my blood oxygen carrying capacity (hematocrit) blood test increased from 42% to 46.4% resulting in a 6% increase in hematocrit/hemoglobin curve as shown on the chart below. EPO medical texts indicate that if I stayed at altitude my hematocrit would continue to increase for 3 to 4 weeks, then level off. Keep in mind that 50% is the max ICU hematocrit value and it may be unsafe to develop a higher reading.
A separate and possibly the greatest benefit from altitude training is the increased white blood count, more than 20% above normal sea level values. The following article is from Runners Web http://www.runnersweb.com/running.html :
Durban, South Africa - Durban Researchers at the University of Natal Medical School have found a link between exercise and an athlete's vulnerability to infection. The studies have determined that too much exercise can begin a process of destruction in up to 85% of the lymphocytes or white blood cells that are responsible for immunity in the body. The finding by a team from the medical school, including Professor Maurice Mars, head of physiology, biochemist Anil Chuturgoon, and masters student Sumen Govender, will be published in an international medical journal. "At Comrades' Marathon time there is big fear among runners that they will get the 'flu or a chest infection," said Professor Mars. He said it was well known among sportsmen that at the point where they are highly trained they become more vulnerable to illness. The team subjected a group of trained sportsmen to intense exercises to the point of exhaustion. Close analysis of the blood cells revealed that a process of apoptosis had begun in 85% of the lymphocyte cells. Apoptosis is a natural process of cell death in which the cells shrink and then break into minute pieces and are eaten by adjacent cells.
See Chart below and references for more information.
Thanks to the staff of UC Barcroft Lab http://www.wmrs.edu/ for their kindness in helping me with my experiment.
A good source for information is the Univ Calif San Diego Medical Library in La Jolla, CA.
These Websites also offer information:
http://www4.nau.edu/hastc/ High Altitude Sports Training Complex of Northern Arizona University
CBC Complete Blood Count and Retic Count.
WBC White Blood Cell Count (Leukocytes) (Neutrophils 55-70%, Lymphocytes 20-40% [both T-cells and B-cells], Monocytes 2-8%, Eosinophils 1-4%, Basophils 0.5-1.0%) The major function of the WBC’s is to fight infection and react against foreign bodies or tissues. Five types of WBC’s are easily identified on a routine blood smear. All these blood cells arise from the same stem cells within the bone marrow as the red blood cell (RBC) does.
RBC Red Blood Cell Count (Erythrocyte Count) This test is a count of the number of RBCs in 1 mm of the peripheral venous blood. The RBC is routinely performed as part of a complete blood count. Packed within each RBC are molecules of hemoglobin that permit the transport and exchange of oxygen and carbon dioxide. Normally, RBCs exist in the peripheral blood for approximately 120 days. Persons living at high altitude have increased RBCs.
HGB Hemoglobin (Hb, Hgb) concentration is a measure of the total amount Hgb
HCT Hematocrit (Hct, packed blood cell volume, Packed Cell Volume [PCV]) The Hct is a measure of the percentage of red blood cells (RBCs) in the total blood volume. It is routinely performed as part of a complete blood count. Therefore the Hct closely reflects the hemoglobin (Hgb) and RBC values. The Hct in percentage points usually is approximately three times the Hgb concentration in grams per deciliter when RBCs are of normal size and contain normal amounts of Hgb. Normal values also vary according to gender and age. Normal findings - Males: 42 to 52%, Female 37 to 47%, Elderly: values may be slightly decreased, Child: 31 to 43%, Infant: 30 to 40%, Newborn: 44 to 64%.
MCV Mean Corpuscular Volume, derived by dividing the HCT by RBC, (HCT/RBC), a measure of average size of a single red blood cell.
MCH Mean Corpuscular Hemoglobin, derived by dividing the HGB by RBC (HGB/RBC), a measure of the average amount (weight) of hemoglobin within an RBC,
MCHC Mean Corpuscular Hemoglobin Concentration, derived by dividing HGB by HCT, (HGB/HCT), a measure of the average concentration or percentage of hemoglobin within a single RBC.
RDW Red Blood Cell Distribution, indication of variation in red blood cell size using MCV and RBC.
MPV Mean Platelet Volume (MPV) The MPV is a measure of the volume of a large number of platelets determined by an automatic analyzer. MPV is to platelets as MCV is to the red blood cell.
Platelet Thrombocyte Count The platelet count is an actual count of the number of platelets (thrombocytes) per cubic milliliter of blood. Platelet activity is essential to blood clotting.
Retic Count The Reticulocyte Count is a test
for determining bone marrow function and evaluating erythropoietic (EPO)
activity. This test is also useful
in identifying anemias. A reticulocyte
is an immature red blood cell (RBC) that can be readily identified under a
microscope by the staining of a peripheral blood smear with a supravital
stain. The Reticulocyte Count
represents a direct measurement of RBC production by the bone marrow.
Mosby’s, Diagnostic and Laboratory Test Reference, 4th Edition, Pagana, K.D. Phd, RN 1999 Harcort Health
Sciences Co.
Email: nealhe@home.com
Neal Henderson
POB 301365
Escondido CA 92030-1365
760 739-1011